
4 Causes itchy skin in pregnancy
Intrahepatic cholestasis of pregnancy
Although most cases of pruritus can be attributed to itchy dry skin, there are conditions unique to pregnancy that involve pruritus as a leading symptom. These include :
A-Pemphigoid gestations
Pemphigoid gestationis, formerly known as herpes gestationis, is a rare autoimmune sub-epidermal bullous dermatosis of that shares some clinical and pathogenic features with bullous pemphigoid. Pemphigoid gestationis typically presents during the third trimester, though it can present in any trimester or even after delivery. It manifests with inflammatory skin lesions and severe pruritus. It tends to recur in subsequent pregnancies earlier and with a more severe course. This activity describes the pathophysiology, etiology, evaluation, and management of pemphigoid gestationis and highlights the role of the interprofessional team in the care of affected patients.
B- Pruritic urticarial papules and plaques of pregnancy
Pruritic urticarial papules and plaques of pregnancy (PUPPP) rash is an itchy rash that appears in stretch marks of the stomach during late pregnancy.
While the exact cause of PUPPP rash isn’t known, the stretching of the skin seems to be a trigger for the rash to occur. PUPPP rash occurs in about 1 in every 150 pregnancies.
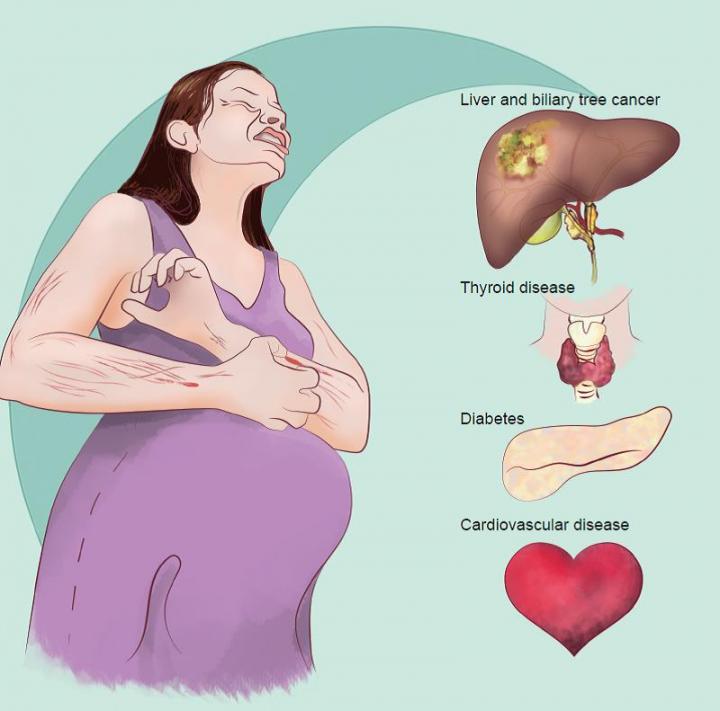
C- Intrahepatic cholestasis of pregnancy
Intrahepatic cholestasis of pregnancy (ICP) is a cholestatic disorder characterized by (i) pruritus with onset in the second or third trimester of pregnancy, (ii) elevated serum aminotransferases and bile acid levels, and (iii) spontaneous relief of signs and symptoms within two to three weeks after delivery. ICP is observed in 0.4–1% of pregnancies in most areas of Central and Western Europe and North America, while in Chile and Bolivia as well as Scandinavia and the Baltic states roughly 5–15% and 1–2%, respectively, of pregnancies are associated with ICP. Genetic and hormonal factors, but also environmental factors may contribute to the pathogenesis of ICP.
Intrahepatic cholestasis of pregnancy increases the risk of preterm delivery (19–60%), meconium staining of amniotic fluid (27%), fetal bradycardia (14%), fetal distress (22–41%), and fetal loss (0.4–4.1%), particularly when associated with fasting serum bile acid levels > 40 μmol/L. The hydrophilic bile acid ursodeoxycholic acid (10–20 mg/kg/d) is today regarded as the first line treatment for intrahepatic cholestasis of pregnancy.
Delivery has been recommended in the 38th week when lung maturity has been established
D- Atopic eruption of pregnancy
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1891276/
ALMOES BLOG


