
Serotonin syndrome
Serotonin Syndrome Alert: Recognizing Early Signs and Ensuring Timely Intervention
Serotonin syndrome is a potentially life-threatening condition caused by serotonergic overactivity due to the use of serotonergic drugs. It can be caused by a therapeutic dose or overdose of a serotonergic drug, concomitant use of multiple serotonergic drugs, or interactions with CYP450 inhibitors. Onset is typically rapid, occurring within 24 hours of drug administration. Classic features include autonomic dysfunction, neuromuscular excitability (e.g., rigidity, hyperreflexia), and altered mental status. Increased neuromuscular activity can also lead to hyperthermia. Serotonin syndrome is a clinical diagnosis but laboratory studies may be used to assess for complications such as rhabdomyolysis. Management involves discontinuation of serotonergic drugs and treatment of features of serotonin syndrome (e.g., agitation, hyperthermia). In most cases, symptoms resolve within 24 hours of cessation of serotonergic drugs. In moderate to severe cases, pharmacological treatment with cyproheptadine may be indicated. Patients with features of severe disease, e.g., life-threatening hyperthermia, may also require sedation and intubation.
Serotonergic drugs
- Antidepressants (e.g., MAOIs, SSRIs, SNRIs, tricyclic antidepressants, vortioxetine, vilazodone, trazodone)
- Anxiolytics (e.g., buspirone)
- Anticonvulsants (e.g., valproate)
- Opioids (e.g., tramadol, meperidine)
- NMDA receptor antagonists (e.g., dextromethorphan)
- 5-HT3 receptor antagonists (e.g., ondansetron)
- Serotonin receptor agonists (e.g., triptans, ritonavir)
- Antibiotics (e.g., linezolid)
- Herbal supplements (e.g., St. John's wort, ginseng, tryptophan)
- Recreational stimulants (e.g., MDMA, cocaine)
Risk factors
- Concurrent use of:
- Two or more serotonergic drugs (e.g., an MAOI with an SSRI)
- One or more serotonergic drug with certain CYP450 inhibitors (e.g., ciprofloxacin)
- Switching from one serotonergic drug to another without tapering
- Accidental or intentional overdose
- Patient-specific pharmacokinetic and/or pharmacodynamic factors
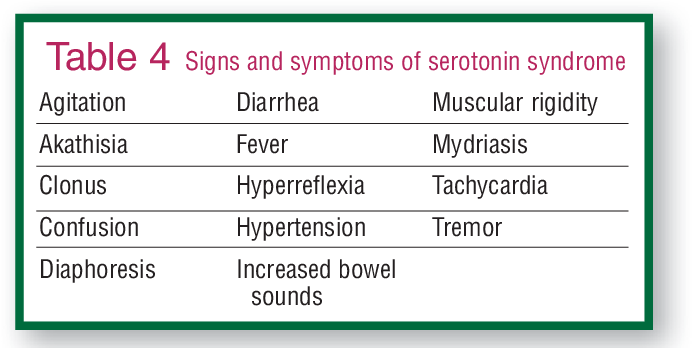
Clinical features
Symptom progression :
- Onset: acute, typically within 24 hours of administration of the causative drug
- Resolution: rapid, typically within 24 hours of treatment initiation
Presentation :
Classic triad:
- Autonomic dysfunction
- Diaphoresis
- Tachycardia
- Hypertension
- Mydriasis
- Neuromuscular excitability: can lead to hyperthermia
- Hyperreflexia
- Myoclonus
- Clonus
- Horizontal ocular clonus
- Hypertonicity
- Rigidity (especially in the lower extremities)
- Altered mental status
- Delirium
- Psychomotor agitation
- Coma
Other features:
- Nausea, diarrhea, vomiting
- Anxiety
- Hypotension (due to MAOI poisoning)
- Seizure
- HAHA! Serotonin syndrome is no joke: Hyperthermia, Autonomic dysfunction, Hyperreflexia, Altered mental status
To differentiate between serotonin syndrome and other drug-induced hyperthermia conditions, remember that only SErotonin Shakes your Extremities (myoclonus and hyperreflexia, mostly of the lower limbs).
Diagnostics
General principles
- Serotonin syndrome is a clinical diagnosis.
- Diagnosis is made based on diagnostic criteria, e.g., Hunter serotonin toxicity criteria.
- Laboratory studies may be used to assess for complications related to muscle rigidity and hyperthermia.
Diagnostic criteria
Presence of any of the following in patients with exposure to ≥ 1 serotonergic drug :
- Spontaneous clonus
- Inducible clonus or ocular clonus plus ≥ 1 of the following:
- Agitation
- Diaphoresis
- Hypertonia and temperature > 38°C (100.4°F)
- Tremor and hyperreflexia
Laboratory studies
- BMP
- ↑ Creatinine in acute kidney injury
- ↓ Bicarbonate in metabolic acidosis
- CBC: ↓ platelets, ↓ Hb, ↑ D-dimer, ↑ aPTT, and ↑ PT in DIC
- ↑ CPK in rhabdomyolysis
- Liver chemistries: ↑ transaminases
Management
All patients
The goal of management is the stabilization of vital signs.
- Discontinue all serotonergic drugs immediately.
- Provide supportive care: e.g., oxygen therapy, IV fluid therapy
- Give symptom-specific treatments.
- Determine severity: For moderate to severe and/or refractory cases, consider treatment with an antidote.
- Mild: tachycardia, hyperreflexia, shivering, diaphoresis, mydriasis, tremor
- Moderate: agitation, hyperthermia < 40°C (104°F), clonus, diarrhea
- Severe: hemodynamic instability, agitated delirium, muscle rigidity, hyperthermia ≥ 40°C (104°F), multiorgan failure
Symptom-specific management
- Agitation and excessive muscle activity: Treat with benzodiazepines.
- Mild symptoms: e.g., low-dose diazepam DOSAGE (off-label)
- Moderate to severe symptoms: higher starting dose, e.g., diazepam DOSAGE (off-label) and repeat doses as needed
- Hyperthermia: Initiate cooling measures, e.g., by reducing ambient temperature, applying cooling blankets or ice packs, administering cold IV fluids.
- Autonomic instability: Use short-acting or titratable medications, as rapid changes in blood pressure and heart rate are common.
- Give antihypertensive treatment.
- Short-acting agents, e.g., esmolol, nitroprusside
- Treat MAOI-induced hypotension or shock.
- Titratable vasopressors, e.g., norepinephrine
Avoid physical restraints, as they can lead to worsening hyperthermia and lactic acidosis.
Moderate to severe and/or refractory cases
- Consider treatment with 5-HT2A receptor antagonists: cyproheptadine DOSAGE (off-label)
- Temperature > 41.1°C: Sedate, paralyze, and intubate patients.
- Use nondepolarizing NMJ blocker as paralytic agent for intubation, e.g., rocuronium.
- See “Endotracheal intubation” for preparation and procedure.
Rule out anticholinergic syndrome prior to administration of cyproheptadine, as cyproheptadine can worsen anticholinergic syndrome.
Avoid bromocriptine and dantrolene, as bromocriptine may worsen symptoms of serotonin syndrome and dantrolene has not been shown to be effective.
Agents other than cyproheptadine, e.g., chlorpromazine, are not currently recommended for the treatment of serotonin syndrome.
ALMOES BLOG


