
Staphylococcal diseases
Staphylococcal diseases
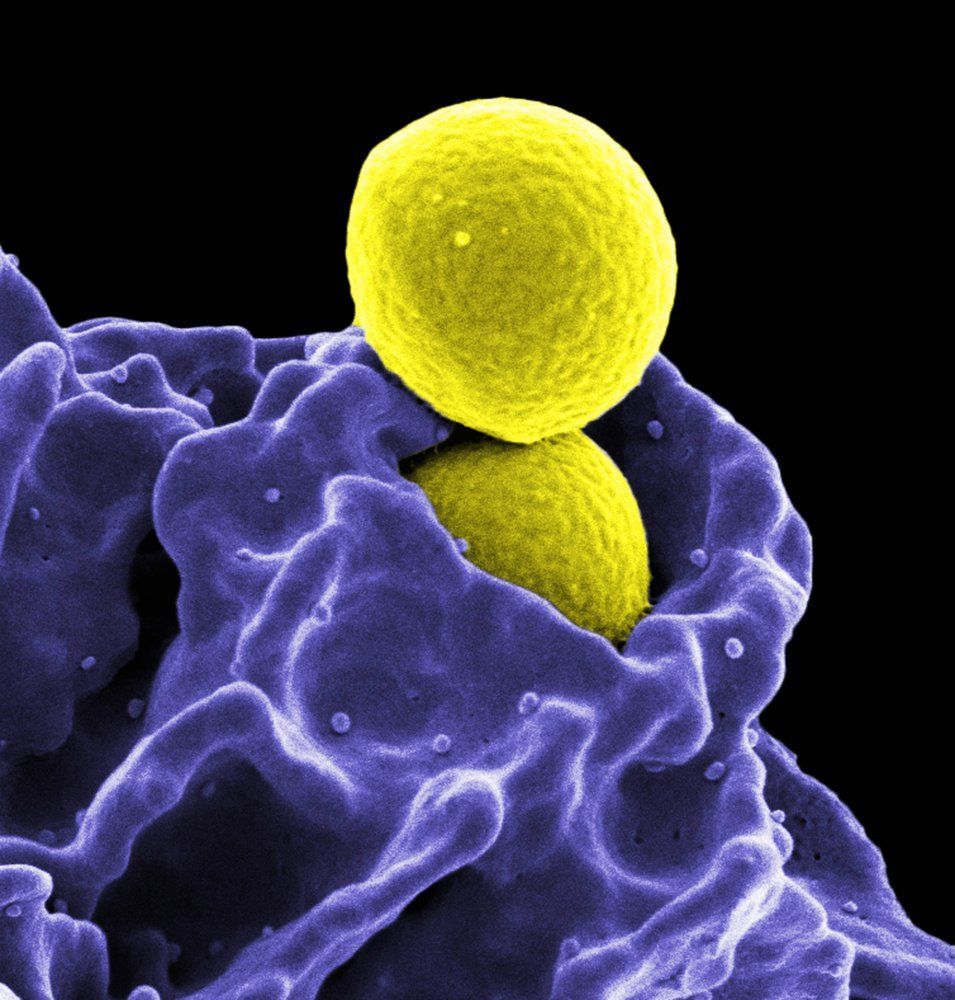
The Staphylococci are gram-positive, spherical-shaped bacteria that form clusters and are commonly found on the skin and mucous membranes. Clinically, the most important species include Staphylococcus aureus and Staphylococcus epidermidis, which are categorized according to their coagulase activity.
S. aureus is coagulase positive and expresses several virulence factors which support evasion of the host immune response.
S. epidermidis is coagulase negative and is usually less virulent, although it can evade the host immune system by forming and subsequently hiding in a biofilm.
S. aureus is commonly responsible for many localized infections (e.g., folliculitis, cervical lymphadenopathy) and also severe organ infections in the setting of bacteremia (e.g., endocarditis, osteomyelitis). As a toxin producer, S. aureus can cause food poisoning (see Staphylococcal food poisoning) and, in severe cases, life-threatening diseases such as staphylococcal scalded skin syndrome (SSSS) or toxic shock syndrome (TSS). Methicillin-resistant S. aureus (MRSA), in particular, poses a major threat to both immunocompromised and multimorbid patients and is a considerable challenge to hospital hygiene.
S. epidermidis is mostly responsible for foreign body infections caused by, for example, contaminated peripheral lines or prosthetic joints. The treatment of choice is anti-staphylococcal penicillins (e.g., oxacillin, flucloxacillin) or first and second-generation cephalosporins..
Treatment :
Staphylococcus aureus
- Anti-staphylococcal penicillins: oxacillin, flucloxacillin
- First and second generation cephalosporins
- In case of penicillin allergy: clindamycin
- MRSA: drugs of last resort such as vancomycin and linezolid
Coagulase-negative staphylococcus (particularly S. epidermidis)
- Methicillin-sensitive: oxacillin, nafcillin, or cefazolin
- Methicillin-resistant: vancomycin or daptomycin
- Second-line treatment (if susceptible): levofloxacin and rifampicin
References
1.
Tong SYC, Davis JS, Eichenberger E, Holland TL, Fowler VG. Staphylococcus aureus Infections: Epidemiology, Pathophysiology, Clinical Manifestations, and Management. Clin Microbiol Rev. 2015; 28(3): p.603-661. doi: 10.1128/cmr.00134-14.| Open in Read by QxMD
2.
Xu SX, McCormick JK. Staphylococcal superantigens in colonization and disease. Frontiers in Cellular and Infection Microbiology. 2012; 2. doi: 10.3389/fcimb.2012.00052.| Open in Read by QxMD
3.
Ghasemian A, Najar Peerayeh S, Bakhshi B, Mirzaee M. The Microbial Surface Components Recognizing Adhesive Matrix Molecules (MSCRAMMs) Genes among Clinical Isolates of Staphylococcus aureus from Hospitalized Children.. Iranian journal of pathology. 2015; 10(4): p.258-64. pmid: 26351495. | Open in Read by QxMD
Source: "ID#: 11155", CDC/ Matthew J. Arduino, DRPH, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
Source: "ID#: 18168", CDC/ National Institute of Allergy and Infectious Diseases (NIAID), Centers for Disease Control and Prevention (CDC) licensed under Public Domain
ALMOES BLOG


